



Introduction
Since the publication of the Flexner Report, medical education has placed a strong emphasis on a scientific approach. Consequently, medical school curricula have adopted the so-called 2+2 system, comprising 2 years of pre-clerkship followed by 2 years of clinical clerkship. This bifurcated curriculum reinforces the idea that basic medical subjects must be taught before clinical training. As a result, students often attempt to integrate and refine their basic medical knowledge in the clinical setting without a comprehensive understanding of the interrelation between these subjects and their application to real patient scenarios.
Medical schools employ a range of methods for clinical clerkship education, including rounds, outpatient preliminary examinations, observations, visits to relevant institutions, attendance at conferences, case presentations, and evaluations of clinical skills. Nevertheless, students sometimes question the value of attending professor-led conferences. Additionally, certain students struggle with the requirement to remain standing in the operating room for extended periods while observing surgeons carry out procedures.
This paper begins by asking how experience in medical school can constitute educational learning. The concept of experience in learning encompasses both learning by doing and learning from experience. Specifically, learning by doing focuses on the methods and processes through which content is acquired through direct action, while learning from experience highlights the significance of personal encounters as a source of knowledge and places the learner at the heart of the learning process [1]. However, the mere presence of experience as the primary source and starting point does not guarantee that all experiences of various natures will result in learning. Learning extends beyond the acquisition of cognitive knowledge; it also involves the transformation of values and attitudes, leading to the adoption of desirable behaviors [2]. In this context, medical education, which is responsible for training future physicians, aims to equip students with the essential qualities of knowledge, skills, and attitudes necessary to perform the duties of a physician. Therefore, it should transcend the mere transmission of knowledge.
This paper attempts to explain the meaning of various teaching and learning methods and activities that students experience, such as clerkships, in medical schools based on experiential learning theory. The importance of experience has been recognized by scholars ranging from Dewey, the pioneer of experiential learning theory, to Kolb, who studied learning with a deep interest in experience, to Sch├Čn, who advocated for reflection on experience as a component of professional education. These scholars have identified reflective thinking as a central component of experiential learning, emphasizing the role of experience as both a catalyst for and a source of learning, the concept of learning as a comprehensive experience, the construction of knowledge through active engagement, and the practical transformation that results from this process.
This paper examines experiential learning theory, which explains how experience leads to learning, and explores its implications for various educational activities in medical schools.
Concepts in experiential learning theory
1. DeweyŌĆÖs continuity and interaction
According to Dewey, learning by experience is driven by two principles: continuity and interaction [3]. DeweyŌĆÖs principle of continuity posits that experiences do not occur in isolation; instead, they are connected to past experiences, which in turn influence and shape future ones. This principle underscores the idea that the significance lies not in the objective phenomena we encounter in the present, but in how these phenomena are perceived and experienced by the individual [4]. Here, the learner adopts an active and proactive stance. Contrary to the behaviorist view that learners are empty vessels to be filled with knowledge or information through education, Dewey suggests that learning happens when the learner integrates existing experiences with new ones [5]. Past experiences influence present ones, which then shape future experiences. Throughout this process, our knowledge is not static but is in a state of constant reorganization.
The second principle is interaction. For an experience to occur, there must be an interaction between the individual and the environment. Interaction refers to the relationship between the external conditions of an experience and its internal factors [4]. This involves a dynamic in which objective and internal conditions converge to create what is known as a ŌĆ£situation.ŌĆØ Life is a process in which an organism continually reconstructs itself through its interactions with the environment, amidst a series of coincidental events. Dewey notes that all humans interact with and adapt to their environment [6]. Adaptation is a means of survival and represents a principle of interdependence. Even those who struggle to adapt to a new society depend on the assistance of others for adaptation, and in doing so, they contribute to the collective existence by supporting others, thus living as interconnected beings.
2. KolbŌĆÖs experiential learning model
Kolb adopted two foundational principles of experiential learning from Dewey: continuity and interaction. According to Kolb, learning is a process whereby knowledge is generated through the transformation of experience. The critical aspect of the learning process is that knowledge is not a static entity to be acquired or transferred; rather, it is a dynamic process of transformation, continuously being created and re-created [7].
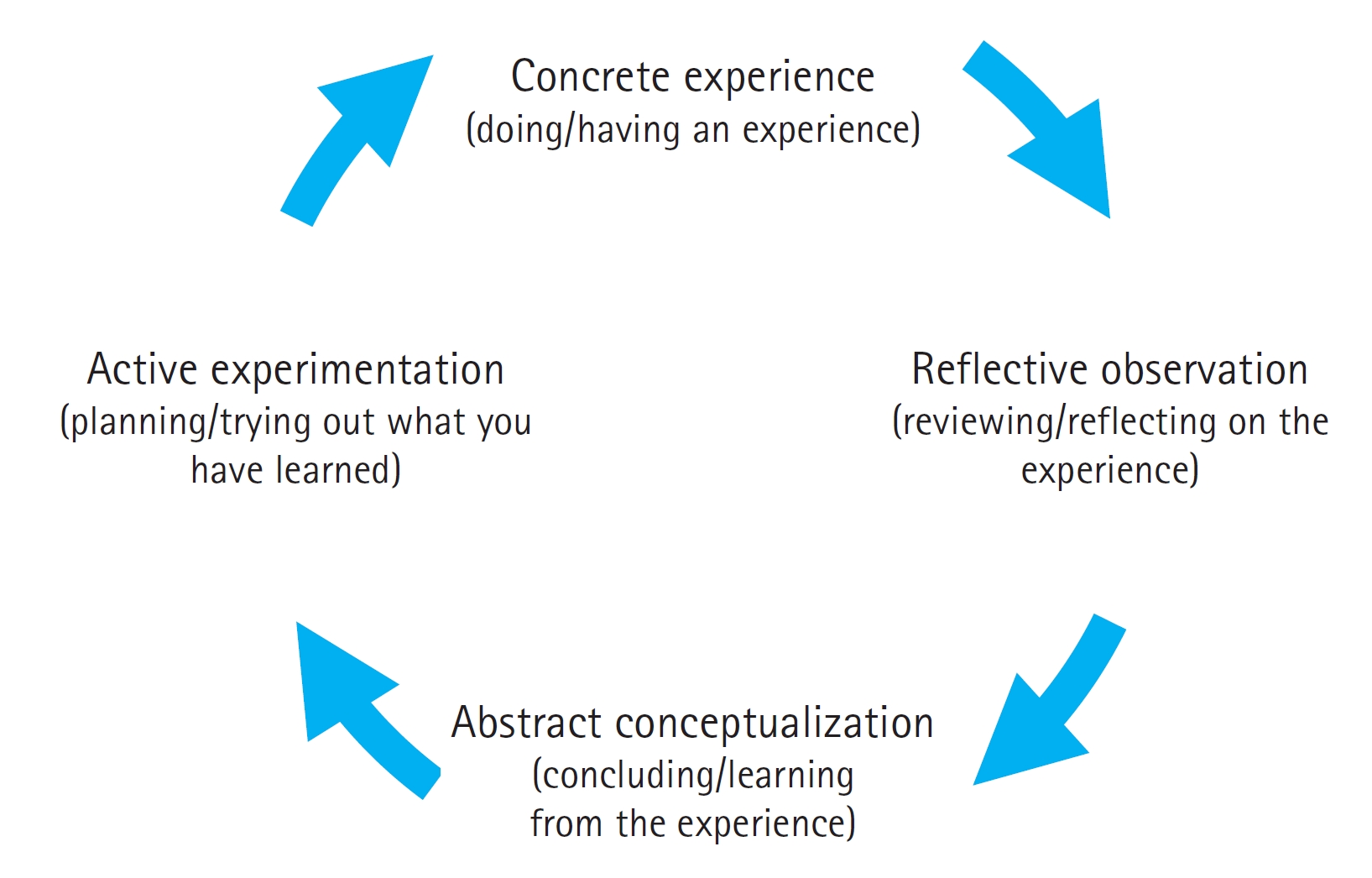
Based on the concept of learning, Kolb [8] proposed a cyclical model of the experiential learning process consisting of four stages. The first stage, concrete experience, involves encountering new and tangible experiences. Not every experience in our daily lives leads to learning; rather, we recognize problems from experiences that either are not well understood, which is a fundamental way of comprehending our environment, or cause emotional discomfort. The second stage is reflective observation, where individuals interpret and reflect upon their concrete experiences in various ways and with differing content. During reflective observation, individuals engage in cognitive reflection to interpret the meaning of the concrete experience that initiated the learning process. The third stage, abstract conceptualization, involves distilling and organizing the insights and principles gleaned from reflective observation. This stage is characterized by logical integration, where the abstract knowledge, principles, and assumptions inherent in the concrete experience are extracted and articulated. Finally, the fourth stage, active experimentation, involves applying the newly acquired theory or knowledge through behavioral experimentation to solve problems and make decisions. The individualŌĆÖs actions in this stage aim to address the problematic situation encountered during the concrete experience stage. The act of proactive implementation itself becomes a new concrete experience for the individual, and should any problematic situation be identified, the individual will sequentially repeat the four processes previously described [9]. KolbŌĆÖs stages of experiential learning are illustrated in Figure 1.
KolbŌĆÖs experiential learning views learning as a process, not an outcome, and as an ongoing process based on experience. This perspective suggests that learning is not merely an activity aimed at achieving a specific result; rather, it is a dynamic process in which learners consistently revise their thinking and behaviors in response to new experiences. Human ideas and thoughts are not static; they evolve continually through interaction with experiences. Furthermore, the learning process is a comprehensive mechanism of social adaptation that involves an interplay between the individual and their environment [10]. In the process of learning, individuals are not passively molded by a static environment; instead, they actively shape their surroundings to meet their own needs. Kolb asserts that learning does not happen through concrete experience alone. It involves a cycle that includes reflecting on the experience, reinterpreting it, and then applying the insights gained to new situations [11]. Without reflection, or if the reflection does not lead to tangible behavior change, an experience cannot be considered true learning. The essence of KolbŌĆÖs experiential learning model is that when individuals encounter new experiences through their senses, they reflect on these experiences, extract lessons, and endeavor to apply these insights effectively in similar future contexts.
3. Sch├ČnŌĆÖs professional education
Learners should engage not only in thoughtful action but also in reflection after the act [5]. Dewey introduced the concept of reflective thinking, differentiating it from daydreaming, dreaming, and the disorganized, vague stream of consciousness. Reflective thinking involves the active, persistent, and careful examination of well-founded beliefs and knowledge, taking into account their origins and potential consequences [9].
The concept of reflection in professional education was emphasized by Sch├Čn [12], who was interested in understanding what sets an expert apart from a novice within a specific professional field and what should be the focus in the education and training of professionals. Sch├Čn [12] posited that professionals require the skill to interpret and manage the situations they face, rather than relying solely on theory-based reasoning. He contended that the ability to accurately read and handle situations cannot be cultivated through theoretical learning alone, as theories are often removed from the situations and contexts in which they originated. Therefore, engaging directly with authentic, real-world situationsŌĆöwhich are inherently complex, uncertain, and variableŌĆöis crucial [12].
Sch├Čn identified a critical skill that separates an expertŌĆÖs proficiency from general competence, which he termed ŌĆ£artistry.ŌĆØ Artistry is not a theoretical skill that manifests in writing or speaking; instead, it is demonstrated through professional conduct. He describes this as ŌĆ£knowing-in-actionŌĆØ or ŌĆ£reflection-in-actionŌĆØ [13]. Sch├Čn categorizes the types of reflection that intervene in the experience-mediated learning process as ŌĆ£reflection-on-actionŌĆØ and ŌĆ£reflection-in-actionŌĆØ [14]. Reflection-on-action is a thorough retrospective analysis of an activity after its completion. Journal writing is a classic example of an activity that fosters reflection-on-action, as it involves a comprehensive review at the end of the day. Through reflection-on-action, we can contemplate the substance of our actions and scrutinize our underlying assumptions, expectations, and presuppositions. Reflection-in-action, in contrast, entails considering different approaches to problem-solving as they emerge during an activity. When confronted with unforeseen issues or events while carrying out a task in the usual manner, it is necessary to identify and implement suitable corrective measures. In essence, reflection-in-action is the mental process of determining the most effective and practical solution to address the problem immediately.
Learning principles of experiential learning theory
In this section, we will explore the implications of key concepts from experiential learning theory for medical education, with a focus on learning principles.
First, according to experiential learning theory, the learnerŌĆÖs entry behavior is considered the starting point of the educational content, which is the learnerŌĆÖs concrete experience [9]. It is essential to identify studentsŌĆÖ entry behaviors and begin from their current state. Specifically, educators should assess studentsŌĆÖ knowledge, skills, and attitudes at the outset. However, some students may be unaware of their entry behavior when they start and may require assistance. Learners should be given the opportunity to recognize what they already know or do not know about the topic at hand.
Second, professional education should commence with concrete rather than abstract methods, unlike general undergraduate education. Concrete methods prove effective when learners lack sufficient prior experience, possess poorly formed concepts about the knowledge they are to acquire, or have limited understanding of the contexts in which the knowledge will be applied. Beginning with concrete methods involves providing learners with hands-on experience, using relevant examples and illustrations, prior to introducing conceptual information. This approach has the benefit of increasing learnersŌĆÖ motivation [15].
Third, the concept of experiential learning places a strong emphasis on reflection within the learning process. New learning emerges from reflecting on experiences, which serve as a foundation for further education. Reflection can be understood as a fresh interpretation of past experiences. As such, it is essential for instructional methods to incorporate the process of recognizing, perceiving, feeling, and thinking in novel ways, as well as seeking solutions to the challenges learners have encountered or the problems they are grappling with. The reflective process entails contemplating the significance of an experience and articulating it in the context of previous experiences. Only through this process can experiences be transformed into practical clinical knowledge applicable in real-world settings. This approach facilitates deep learning that not only enhances understanding but also equips learners for future patient encounters [16].
Fourth, the instructor must act as a mediator, creating opportunities for students to engage in self-directed experiences and ensuring that meaningful learning takes place through proper reflection on those experiences. The instructor should facilitate learning and encourage students to draw connections between the subjects they study. Instructors can promote critical reflection by adopting an approach that enables students to formulate and test their own hypotheses, instead of offering detailed explanations or dictating what is right or wrong. The effectiveness with which an instructor engages students in critical reflection is crucial to successful learning [17].
Fifth, students should have the ability to assess their own grades and progress. Understanding oneŌĆÖs performance is a crucial indicator of effective learning. Equally important is gaining insight into their own strengths and weaknesses. While traditionally, students are evaluated by their instructors, reliance solely on instructor feedback and one-time paper tests may not sufficiently facilitate effective learning. Consequently, students may end up studying merely to pass tests rather than to deepen their understanding through the learning process. Additionally, students may find themselves conflicted between the objectives of formative and summative assessments [15].
Application of experiential learning theory to medical education
1. CoxŌĆÖs experience-explanation cycle of clinical clerkship program
The experience-explanation cycle of clinical training by Cox [18] is characterized by its emphasis on reflective thinking during clinical clerkships. The first experience cycle begins with preparation for the clinical encounter. Prior to the experience, the studentŌĆÖs knowledge is assessed, and preliminary explanations are provided, such as the patient's medical history. Then, the experience commences with exposure to the clinical setting through patient contact. This process encompasses meeting with the patient, discussing the disease, examining physical symptoms, and contemplating patient care. The experience cycle concludes with a debriefing session after examining the patient, and involves reviewing and interpreting relevant materials. The second part is the explanation cycle, which follows the experience cycle and starts with reflection. This reflective process is grounded in a clinical situation that the students have recently encountered. They are encouraged to describe the clinical process from various perspectives. Essentially, they move beyond the experience cycle by engaging in a reflective process to contemplate the significance of the experience and articulate it in the context of prior experiences to enhance learning. This cycle translates into practical clinical knowledge that can be applied in real-world medical practice. The explanation cycle promotes deep learning, which in turn prepares students for future patient encounters [16].
2. Reflective journaling as a pedagogical strategy
Reflective journaling is one of the most common pedagogical strategies for eliciting reflection in education. A reflective journal is a learning tool that allows learners to reflect on themselves and their experiences in the learning process, and to express their feelings and thoughts honestly in writing [19]. Mezirow [20] categorized reflection into three types based on the nature of reflective thinking: reflection on content, reflection on process, and critical reflection. Reflection on content involves examining the substance of an event or issue, primarily by asking ŌĆ£whatŌĆØ questions to gain self-awareness. Reflection on process entails identifying the strategies employed to address the problem, with a focus on self-awareness by asking ŌĆ£howŌĆØ questions. Critical reflection, the most advanced level, is initiated by presenting a problem and involves self-awareness by predominantly asking ŌĆ£whyŌĆØ questions. This level of reflection can lead to a transformation in oneŌĆÖs system of meaning, potentially resulting in conceptual change. For journal writing to serve effectively as a tool for reflection and introspection in medical education, systematic consideration must be given to the type and quality of reflection articulated in the journals [21]. Reflective journals in medical education should aim not only to explain learning content or to facilitate a superficial level of reflection but also to provoke deeper levels of reflection [22,23].
Conclusion
Although there is no doubt that learning activities involving direct patient care are crucial in medical education, there has been limited opportunity to explore which learning theories are integrated into medical school curricula and how these theories can enhance educational practices. Beginning with an inquiry into how diverse experiences in medical education contribute to learning, this paper investigates the experiential learning theories of Dewey, Kolb, and Sch├Čn and discusses concrete examples of their application within the context of medical education.
Experiential learning views learning as being derived from concrete experiences or through active engagement. However, as described by various scholars, while experiential learning certainly prioritizes experience, it places even greater emphasis on the process of reflective thinking. Theories of experiential learning advocate for reflection upon experiences as a means to develop new skills, attitudes, and thought patterns. Learning transpires not solely from the knowledge imparted in lectures but also from the cyclical process of taking action and engaging in reflective thinking. In this paper, we outline five key principles of experiential learning theory. First, it is essential to ascertain the studentsŌĆÖ initial behavior in terms of their knowledge, skills, and attitudes. Second, the learning material should be structured to move from tangible, concrete experiences to more abstract concepts. Third, the learning process must incorporate reflection. Fourth, the instructor should serve as a facilitator, helping to immerse the student in the experience and render it significant. Last, students should have the opportunity to assess their own learning progress.
Based on our discussion of experiential learning theory we would like to suggest the following directions for medical education from an educational perspective.
First, in accordance with the principles of continuity and interaction in experience, medical education programs should facilitate experiential learning, enabling learners to reconstruct and reflect upon their experiences. Medical professionalism is best developed within authentic medical contexts, such as during rounds, in clinics, through service, and via activities tailored to specific learning objectives. It is essential for learners to engage with a diverse array of experiences, both in classroom settings and clinical environments. Through observation and reflection, often within broader learning communities, they can assimilate these experiences. This process allows them to formulate their own theories, deepen their understanding of the world, and enhance their capacity for learning in novel ways [24].
Second, there is a need for a systematic approach to teaching and learning that integrates reflective thinking into medical education. Dewey, Kolb, and Sch├Čn all emphasized the role of reflective thinking in the learning process. Reflective thinking is essential for transforming experiences into learning and knowledge. Medical educators must consider and investigate ways to weave reflective thinking into the fabric of the learning process. To elevate the current state of clinical clerkship education, as described in the introductionŌĆöcharacterized by hospital observationsŌĆöinto a truly educational experience, a grasp of experiential learning theory and a more systematic learning design are necessary.
Medical education is changing rapidly. Medical schools have the mission of preparing physicians who are not only competent but also capable of fulfilling their professional roles in an unpredictable future. Therefore, integrating the principles of experiential learning theories into medical education is significant for the professional development of future physicians.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



