



Introduction
Medical students consistently manage to absorb a substantial amount of information every day [1]. What processes are occurring in their brains during this learning? What exactly happens when learning takes place, and what are the implications? How can educators effectively engage with and influence the learning process? The field of psychology has been exploring these questions for some time, and as a result, educators have formulated a range of teaching strategies that translate learning theories from research settings into practical classroom applications. Contemporary medical school curricula are moving away from traditional lecture-based formats toward more interactive discussions and participatory learning experiences. Furthermore, there is a paradigm shift underway in medical education, moving from a subject-oriented, discipline-centered approach to one that is problem-based, clinical-presentation-oriented, and schema-focused [2]. These changes are the result of medical schools' adoption of various educational theories, aiming to meet contemporary needs and enhance educational effectiveness. Historically, major learning theories have laid the groundwork, providing both the theoretical underpinnings and the methodological frameworks that have guided the evolution of medical education [3,4].
Theories on learning were predominantly behaviorist in the early 20th century, then shifted towards cognitivism in the mid-20th century, and today, constructivism is the prevailing trend. Behaviorism posits that learning occurs through a combination of stimuli presented to an organism and the organismŌĆÖs responses, whereas cognitivism asserts that learning takes place through mental processes within an organism, without the need for environmental stimuli. Constructivism, in contrast, has criticized both theories for their reliance on objectivist epistemology. It argues that learning is not about acquiring knowledge that is objectively proven to be important, but rather about learners constructing knowledge that is meaningful to them [2,4]. Despite the shift in todayŌĆÖs educational paradigm, the educational approaches derived from behaviorism and cognitivism remain valuable in schools.
Among learning theories, cognitivism focuses on mental processes such as perception, cognition, attention, encoding, and memory, and has proposed various principles for teaching and learning [4]. Cognitivism has been applied to numerous subjects that require scientific thinking, problem-solving skills, an understanding of natural and scientific concepts, and the acquisition of expertise [5,6]. In medical education, it has provided a theoretical foundation for problem-based learning and organ-based curricula [3,4]. Medical educators have consistently sought to identify suitable teaching methods and strategies from various educational theories [4]. The present study aims to examine cognitivist theory to identify strategies that can be effectively used in medical education and to present real-world case studies of teaching.
The application of cognitive theories to medical education is justified for two primary reasons. First, the development of studentsŌĆÖ thinking skills in medicine necessitates the efficient memorization of a vast body of medical knowledge [4]. Cognitivism, which offers a range of learning strategies for the input, processing, and storage of knowledge, may provide suitable teaching strategies to alleviate the learning burden on medical students. Secondly, one of the main educational objectives of medical schools is to produce professionals adept at problem-solving and clinical reasoning [4]. Cognitivism, with its strategies for systematizing and organizing knowledge and for understanding the thought processes of experts [4], can offer teaching strategies that align with the goals of medical education. Therefore, this study does not aim to provide a detailed theoretical explanation of all teaching theories encompassed by cognitivism. Instead, it aims to present specific teaching strategies and classroom examples that will enable instructors to implement cognitivist teaching strategies in their courses. Specifically, first, the present study intends to examine cognitivist theory from the perspective of teaching methods rather than psychology. This approach is taken because the psychological perspective is concerned with explaining the experimental and theoretical principles of learning, cognition, and memory, whereas the teaching method perspective focuses on how to apply cognitivist principles in educational settings. Second, this study selects and presents cognitivist teaching principles that are suitable for the content taught in medical schools. Third, by presenting real-world cases, the present review aims to demonstrate how teaching strategies can be applied in the classroom.
Cognitive learning theories encompass a range of perspectives on how learning occurs. Social cognitive theory suggests that learning is a product of social interaction. Gestalt theory proposes that learning arises from insights into forms or patterns. PiagetŌĆÖs developmental cognitivist theory posits that learning is a function of the development of cognitive structures at various developmental stages. Information processing theory draws parallels between human learning and computer information processing, aiming to elucidate the human learning process [7]. This study focuses on cognitive learning theories from an information processing standpoint. It includes the information processing theory by Atkinson and Shiffrin [8], which outlines a model of cognitive processing; cognitive load theory, which examines the interplay between cognitive load and learning and offers strategies to mitigate cognitive load [9,10]; and schema theory, which contends that memory is structured around cognitive frameworks known as schemas. According to schema theory, new information and experiences are meaningfully integrated into memory when these schemas are well-organized [11]. The literature reviewed for the present study included books, research papers, and dissertations on cognitivist learning theory, cognitive science, and teaching-learning methods related to thinking. For teaching cases applied to medical schools, I selected studies that presented teaching methods and results from the results of PubMed and Google Scholar searches for ŌĆ£cognitivism,ŌĆØ ŌĆ£cognitive theory,ŌĆØ ŌĆ£imagination,ŌĆØ ŌĆ£schema,ŌĆØ ŌĆ£concept map,ŌĆØ ŌĆ£meta-cognition,ŌĆØ ŌĆ£medical education,ŌĆØ or ŌĆ£medical school.ŌĆØ Among these, I selected practical classroom examples that could realistically be applied in medical schools.
The background of the emergence of cognitive learning theory
Cognitive learning theory emerged in response to the critique that behaviorism did not fully account for all aspects of human learning. Behaviorists posited that human consciousness impeded the study of behavior, treating the mind as an impenetrable ŌĆ£black boxŌĆØ and attributing changes in behavior to observable actions external to the mental realm [12]. Behavioral learning theory is rooted in John B. WatsonŌĆÖs seminal 1913 paper ŌĆ£Psychology as the behaviorist views it,ŌĆØ drawing on Ivan PavlovŌĆÖs work on classical conditioning as evidenced by salivation in dogs, Edward ThorndikeŌĆÖs puzzle box experiments with cats, and B.F. SkinnerŌĆÖs operant conditioning experiments involving pigeons and rats pressing levers for food rewards. According to behaviorists, behavioral changes occur not because of cognitive processes such as beliefs, knowledge, or reasoning, but rather due to external stimuli, rewards, and environments. Learning is defined as a process of trial and error, where an external stimulus (S) elicits a response (R), which is then reinforced and conditioned. The use of praise, stickers, rewards, punishments, and programmed learning in educational settings are enduring examples of behaviorist principles in action [12-14].
Despite behaviorismŌĆÖs scientific approach to objectively studying learning behavior, cognitivism emerged, challenging the notion that human behavior can be fully explained by stimulus-response associations alone. In the 1900s, as behaviorism dominated American psychology and education, a new perspective on learning surfaced within German psychology. This was the work of the Gestalt psychologists, who concentrated on the mental processes that behaviorists dismissed as the ŌĆśblack boxŌĆÖ and consequently excluded from their studies. Max Wertheimer, along with colleagues K├Čhler and Koffka, is often referred to as the founder of Gestalt psychology following his publication on the apparent motion in 1912. While on a train journey, Wertheimer observed two alternating lights that seemed to move, leading him to the realization that humans tend to perceive objects as integrated wholes rather than as isolated parts. He termed this the ŌĆśphi phenomenonŌĆÖ and noted that the perception of motion cannot be explained by examining the lights in isolation. This insight became a core principle of cognitivism: the whole is greater than the sum of its parts, and to divide is to distort. The Gestalt psychologists, much like the behaviorists, contended that ŌĆśhuman behavior as a wholeŌĆÖ cannot be fully comprehended if one attempts to dissect ŌĆśbehaviorŌĆÖ into separate ŌĆśstimulusŌĆÖ and ŌĆśresponseŌĆÖ components [12-14]. K├ČhlerŌĆÖs experiments, published in 1917 under the title ŌĆ£The Mentality of Apes,ŌĆØ revolutionized our understanding of the learning process. Conducting his research at the Berlin Institute for Ape Research on an island in the Canary Islands, located off the coast of Northern Africa, he devised a series of experiments involving monkeys. In one experiment, he suspended a banana at an unreachable height above the monkeysŌĆÖ cage and provided several boxes and sticks within the enclosure. Initially, the monkeys were unable to reach the banana. However, they eventually had a moment of insight, or what is often referred to as the ŌĆ£Aha-experience,ŌĆØ when they stacked the boxes to successfully retrieve the banana. This experiment demonstrated that an organism's behavior can be altered not only by external stimuli but also through internal cognitive processes [14]. This study shifted the paradigm of learning theory from behaviorism to cognitivism.
With the advancement of computer science in the 1950s, the information processing theory emerged, drawing parallels between human learning processes and computer information processing. This theory posits that human memory and thought structures, as well as memory and thought processes, are analogous to the way computers process information. It conceptualizes the human learning process as an input-processing-output sequence [14]. This perspective sought to explain the processes occurring within ŌĆ£insight.ŌĆØ Numerous scholars have proposed models describing how information is received by the human brain, processed, and then stored in long-term memory. Repovs and Baddeley [15] introduced a model of working memory that outlines the components of working memory and its function in processing incoming information. Atkinson and Shiffrin [8] proposed a three-stage memory model, suggesting that external stimuli are transferred to long-term memory through three ŌĆ£buckets,ŌĆØ or memory stores. Sweller [9,10] explained the mental load of information processing and its relationship to learning through the cognitive load model. Furthermore, Bartlett [11] presented a schemata related to long-term memory and retrieval. These information processing models attempt to explain how humans store information in memory, how stored information is transformed, and how it is retrieved from memory.
Cognitive load theory has been applied in medical schools [4,6,16-19], particularly in subjects that demand extensive memorization, such as anatomy and pathology [4], as well as in complex tasks that require novice students to perform at the same level as experts, and in authentic tasks that integrate medical knowledge, skills, and attitudes [17]. According to these studies, in subjects associated with high cognitive load, it is essential for instructors to design a learning environment that minimizes the cognitive load for learners.
Learning perspective and learner perspective
In cognitive learning theory, learning results from the effective organization and processing of incoming information via internal mechanisms. As the human brain receives information through the sensory organs, learning takes place through a series of processes: attention, recognition, encoding, and memory. Thus, this sequence of processing steps constitutes the learning process, with the information retained being regarded as the learning outcome [5].
In a classroom setting, students typically listen to a professorŌĆÖs lecture to acquire knowledge, a process referred to as behaviorism. Within this framework, learners are viewed as ŌĆ£blank slateŌĆØ and passive recipients of knowledge (external stimuli) [13,14]. Conversely, cognitivism posits that learners are self-directed individuals who actively organize their cognitive structures. As such, while the instructor's role in behaviorism is to impart knowledge, in cognitivism, it is to foster a meaningful classroom environment and facilitate cognitive strategies that enhance the learners' processing of information [13,14].
Learning process based on the information processing model
Atkinson and Shiffrin [8] proposed a theory of human learning and memory based on the information processing model. This theory posits that when learners receive stimulus information from the environment through their sensory receptors, the information is transferred to short-term memory and then to long-term memory. Here, it is encoded, stored, retrieved, and responded to, culminating in the process of learning (Figure 1).
The sensory register receives and processes incoming stimuli from the human senses. Information that enters the sensory register is lost within two seconds unless further cognitive activities are engaged. Some of this information is recognized again, or given selective attention, and then transferred into short-term memory (Figure 1). Recognition involves pattern recognition, where the learner associates incoming stimuli with information stored in long-term memory. Selective attention involves focusing on specific information while inevitably ignoring other stimuli, enabling the perception of a particular piece of information [20].
Working memory, also known as short-term memory, serves as the conscious processing space for both retrieved long-term memory data and newly acquired information, utilized in problem-solving tasks. This cognitive function temporarily holds the necessary information for immediate use. Analogous to a computerŌĆÖs RAM [10], working memory is a mental workspace where critical learning activities, such as problem-solving, decision-making, and the manipulation and organization of information, take place [5]. The capacity of working memory is finite. While individual differences exist, it is generally accepted that the maximum amount of information it can hold at one time without external aids is around 7┬▒2 items [21]. Without repeated rehearsal, information is lost within about 30 seconds [21]. To counteract this limitation and preserve information for extended durations, strategies like chunking (organizing information into meaningful groups), achieving automaticity (streamlining the processing of information), and employing dual processing are employed. Information within working memory interacts with that retrieved from long-term memory. During this interaction, some information may be lost, while other pieces are organized, elaborated upon, and transformed through mental imagery. This process facilitates meaningful learning and the eventual storage of information in long-term memory.
Long-term memory serves as a repository where information is encoded and stored for an extended period, potentially indefinitely. This information is organized into semantic and episodic knowledge, forming schemasŌĆönetworked structures that organize information. The knowledge retained in long-term memory is acquired through learning and is accessed via search and retrieval processes when needed [20].
Seven cognitive teaching strategies
Effective classroom learning occurs when the instructor understands the learnersŌĆÖ internal cognitive processes and creates an environment that supports their cognitive processing [20]. Several studies [5,6,14,18,22-24], the ŌĆ£Instructional guidelines for improving studentŌĆÖ learningŌĆØ proposed by the American Institute of Education Sciences [25], ŌĆ£Cognitive load theory: implications for medical educationŌĆØ published by the Association for Medical Education in Europe (AMEE) [20], and ŌĆ£Clinical teaching strategies for clinical instructors [26]ŌĆØ propose cognitive teaching strategies that can be utilized in medical schools. Drawing from these sources, Table 1 presents seven teaching strategies along with specific activities that can be applied according to the learnersŌĆÖ information processing. These strategies are categorized as follows: (1) strategies to facilitate the reception of learning materials, (2) strategies for concentrating and distributing attention to enhance learning retention, (3) strategies to reduce cognitive load, (4) encoding strategies, (5) information retrieval strategies, (6) distributed learning strategies, and (7) metacognitive strategies.
1. Strategies to facilitate the reception of learning materials
Strategies that facilitate the reception of learning materials are those that activate the learning process [7]. Learning begins when the instructor introduces material that aligns with sensory information, which the learner then perceives or receives. At this initial stage, it is crucial for the instructor to present the material in a manner that is readily perceptible to the learner. For instance, at the start of a lesson, the instructor might present a quiz on the key concepts to be memorized, or provide audiovisual materials or clinical cases that are pertinent to the lessonŌĆÖs content (Table 1).
2. Strategies for concentrating and dividing attention for learning retention
Strategies for concentrating or dividing attention help maintain an appropriate level of learner engagement after the initial learning trigger, ensuring continued learning or task performance [7]. Instructors can choose from different strategies tailored to four distinct types of attention [6]. Firstly, selective attention strategies enable learners to concentrate on relevant information while disregarding distractions. Secondly, divided attention strategies assist learners in appropriately distributing their focus when managing multiple tasks simultaneously. Thirdly, arousal strategies are employed to keep learners vigilant during extended learning sessions. Lastly, executive attention strategies are crucial for sustaining focus to successfully complete a task. Table 1 presents specific techniques that can aid learners in focusing or managing their attention. It is crucial to acknowledge that individual differences may influence learnersŌĆÖ preferences for attentional strategies and their capacity to maintain attention [27].
3. Strategies for reducing the cognitive load to minimize the cognitive burden
Cognitive load refers to the total demand placed on a learnerŌĆÖs cognitive system during a specific task [6]. A strategy for reducing cognitive load involves instructors tailoring the level of demand to minimize unnecessary cognitive strain on learners [7,16]. Within the human cognitive system, working memory serves as a critical bottleneck in learning, as it can process only a limited amount of information at any one time [20]. According to cognitive load theory, the types of cognitive load experienced in short-term memory are categorized into three distinct types, and their combined magnitude must not surpass the capacity of short-term or working memory [28]. These include intrinsic load, which arises from the inherent difficulty or complexity of the task; extraneous load, which results from the instructional approach, including the nature of teaching materials and the method of presentation; and germane load, which is influenced by individual differences such as learnersŌĆÖ cognitive strategies [16]. As an instructor, you have the ability to modulate both intrinsic and extraneous loads through the application of effective teaching strategies. Instructors can alleviate cognitive load for learners by presenting learning materials, complex tasks, examples, or multimedia resources in a manner that aligns with the learnersŌĆÖ needs [9,16].
4. Encoding strategies for retention
Encoding is the process by which information is transformed from its visual representation in working memory into a format that can be stored in long-term memory [5]. For learning material to be retained in long-term memory, it must be encoded in a form that has meaning. The level of processing theory posits that information processed at a deeper level, which involves giving personal significance to the material, is more likely to be remembered than information processed at a superficial level, which merely involves recognizing or naming the material as it appears [6]. Deep processing can be categorized into three strategies: elaboration, organization, and imagery. Elaboration deepens understanding by connecting new information to existing knowledge [25]. Organization involves logically restructuring the relationships between elements of the material to enhance comprehension. Imagery entails creating mental images to represent information, which could be visual, auditory, or tactile in nature. Encoding strategies, therefore, refer to instructional methods that employ elaboration, organization, and imagery to aid learners in effectively retaining content. Specific methods are presented in Table 1.
5. Strategies for retrieving learned information
Recognizing learned information in long-term memory is known as retrieval [28]. Retrieval exerts a more significant influence on learning outcomes and memory than any other strategy [28]. Instructors can enhance the effectiveness of retrieval by encouraging students to actively generate sensory, cognitive, or emotional cues [28]. For facilitating retrieval, it is more advantageous to recall information in context or alongside words that are readily associated with it [5]. Internal states also impact retrieval; memory is more effectively activated if the mood or emotional state during retrieval matches that at the time of encoding [5]. Instructors should consider this and promote the development of retrieval strategies in the classroom (Table 1).
6. Distributed learning strategies for enhancing memory retention
Retention refers to the ability to maintain stored information in long-term memory over an extended period [6]. Information is more likely to be remembered for a longer duration when it is learned over time through distributed learning, as opposed to being crammed into a single session. As an instructor, one has the option to select and implement distributed learning strategies to enhance the retention of learners (Table 1).
7. Metacognitive strategies for managing cognitive strategies
Metacognition is cognition about cognition, which refers to strategies for monitoring oneŌĆÖs own learning and planning, selecting, and evaluating the use of necessary cognitive strategies [26]. Learners must develop efficient cognitive strategies to construct knowledge independently and become lifelong learners. Ineffective cognitive strategies can lead to difficulties in situations that demand intensive study and the integrated application of knowledge [29]. An instructor can offer targeted support to assist learners in mastering their cognitive strategies (Table 1).
Cognitive learning theory and instructional design
Gagn├® [30] proposed a teaching theory that applies cognitive learning theory to actual classes. He defined a class as ŌĆ£a set of external environmental events that are intentionally designed and arranged to support the learnerŌĆÖs internal processesŌĆØ [30]. Based on this definition, he proposed nine ŌĆ£events of instructionŌĆØ that instructors can apply to maximize studentsŌĆÖ outcomes based on the learner's cognitive processes. It is not necessary for an instructor to employ all nine events of instruction in every class; rather, they can be selectively adapted or modified to suit the specific context of the class.
In the introductory step of a class, the instructor can use the following strategies: (1) gaining attention and (2) informing the learners of objectives. In the development step of a class, the instructor can use (3) stimulating recall of prior learning, (4) presenting the new content, (5) providing learning guidelines and directing learning, (6) providing exercises and learning activities, and (7) Providing feedback on classroom activities. At the end of class, lesson summaries can be used to (8) provide a formative assessment of what was learned in class, and (9) enhance retention and transfer [29]. Instructors can prepare lesson plans according to the standards presented in Table 2.
Writing a syllabus is analogous to writing a movie script before making a movie [31]. Although the script is prepared in advance, it remains flexible and can be adapted during filming, providing a clear direction for the project. In the same way, developing a syllabus before the class offers a roadmap for the courseŌĆÖs progression. The structure of the syllabus is outlined in Table 2. Furthermore, to determine the necessity for teaching strategies and syllabus design, the cognitive processes of learners, teaching strategies, and the significance of the syllabus are illustrated together in a single diagram from a cognitivist perspective (Figure 1).
Designing the curriculum based on a cognitivist perspective
1. Objective of education
The implications of a cognitivist perspective for curriculum design were examined from a cognitivist perspective. Peterson et al. [32] proposed a reform plan for secondary education in the United Kingdom, suggesting that the goal of education, according to cognitivism, is to facilitate the use of various intellectual activity modalities rather than merely transmitting knowledge. Lee [33] categorized these intellectual activities as empirical, logical, aesthetic, and moral. The objective across all subjects is to learn cognitive rules through the curriculum content and to develop the ability for free intellectual activity. The focus of education should be on acquiring ŌĆ£cognitive knowledge,ŌĆØ meaning that the curriculum ought to be structured around ŌĆ£knowing howŌĆØ instead of ŌĆ£knowing that.ŌĆØ Teaching methods, therefore, should prioritize thought processes and aim to foster cognitive activities [33]. Viewed from this angle, the current medical curriculum can be assessed as a competency-based curriculum designed to develop practical abilities, aligning with the principles of cognitivism.
2. Curriculum design principles
The AMEE presented 12 points to consider in curriculum design from a cognitivist perspective [34]. They highlighted three main aspects. First, it is important to consider task fidelity and organize content in a manner that minimizes cognitive load or emotional difficulty. For instance, in planning medical interview practice, the sequence should be structured to have students engage with simulated patients before progressing to interactions with real patients. Second, instructors should consider task complexity and sequence tasks from those with lower cognitive difficulty to those with higher cognitive difficulty. Third, as cognitive load or task complexity rises, instructional and environmental support should be correspondingly increased to aid learners.
Exemplary cases of cognitive teaching strategies
1. Blank page anatomy lesson with metacognitive strategies
This teaching method was developed for a first-year anatomy and physiology course at the Queensland University of Medical Sciences in Australia, and it promotes metacognition [35]. The duration of the course was 14 weeks, with 3 hours of class time every 2 weeks (21 hours total). Between 120 and 150 students were divided into 15 to 18 groups to study at 6 to 8 anatomy stations. These stations were set up in a small group discussion room. The classroom was referred to as a ŌĆ£blank pageŌĆØ because it was devoid of learning resources, equipped only with a blank chalkboard.
The teaching method involved students entering a station and either sculpting with clay or drawing a specific anatomical structure as directed by the tutor. During the initial 3ŌĆō5 minutes of the activity, students attempted to recreate the anatomy without any instructional aids. Subsequently, they refined their work with the assistance of the tutor and various learning materials to accurately complete the structure. Each station experience lasted between 15 and 20 minutes, after which students proceeded to the next station upon completion. Rather than providing direct answers, the tutor facilitated the studentsŌĆÖ independent recall of the information. The assessment consisted of a 10-minute quiz at the conclusion of each 3-hour session. The classroom setting and layout are depicted in Figure 2.
On the formative assessment quiz, students in the ŌĆ£blank pageŌĆØ class achieved marginally higher scores compared to those who received a review of anatomical structures. In a subsequent satisfaction survey, students described the method as ŌĆ£fun, thought-provoking, and motivating.ŌĆØ They rated the approach as satisfactory and worthy of recommendation. In conclusion, this method fostered metacognitive skills in students and promoted visual and spatial reasoning, which facilitated deep learning. Furthermore, students positively appraised the method, finding it non-threatening and valuable for long-term retention. They attributed these benefits to the methodŌĆÖs encouragement of deep learning through the use of multiple symbols for description and creation.
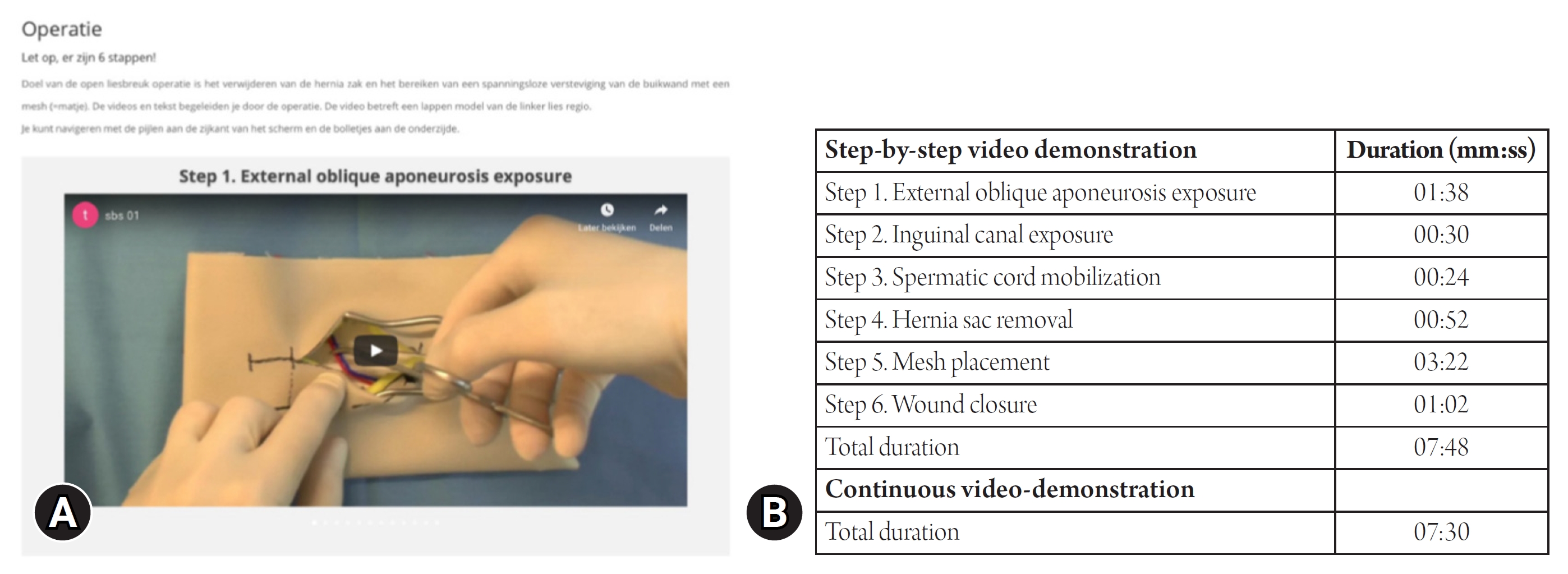
2. Step by step video-based learning for applying cognitive load reduction strategies
This method involved video-based instruction to prepare medical students for performing surgical procedures and was implemented at Erasmus University Medical Center in the Netherlands in a non-regular surgical skills training class [16]. Students practiced the Lichtenstein open inguinal hernia repair (LOIHR) by following along with a video. The instructional video, which was 7 minutes and 30 seconds long, detailed the procedure in six distinct steps rather than presenting it as one continuous segment (Figure 3). The videos were structured in a ŌĆ£step-by-stepŌĆØ format, with each segment demonstrating and explaining the corresponding part of the procedure in detail. The study's findings indicated that the extrinsic cognitive load associated with the segmented documentation method was lower compared to that experienced by students who learned through continuous video demonstrations. Furthermore, in the actual performance assessment, students who were taught using the step-by-step method not only scored higher but also committed fewer errors than those who learned through the continuous demonstration method.
Conclusion
Educational theory has played an important role in the ongoing development of medical education. In particular, cognitive learning theory is one of the major educational theories that studies human thought processes. This study explored the educational implications of cognitive learning theory for today's medical education and proposed teaching strategies that can be practically applied in the field. In addition, it is hoped that the present review will narrow the gap between theory and practice by presenting classroom examples of applying cognitive teaching strategies.
In this study, I presented cognitive teaching strategies and principles that can be applied in medical schools across three distinct areas. Initially, I provided teaching strategies and specific examples tailored to the learner's stage of cognitive processing, enabling instructors to seamlessly integrate cognitivist learning theory into their classroom instruction. This material allows instructors to readily incorporate one or two teaching strategies into their existing classes. Next, I introduced a cognitive lesson design plan to assist instructors in systematically organizing their lessons. This plan includes nine instructional ideas and examples that can be directly applied in the classroom setting. Utilizing this framework, instructors can strategically plan their lessons to enhance their effectiveness. Lastly, I discussed cognitive design principles that curriculum development teams should consider when creating a curriculum, which is a broader entity than an individual lesson. For instance, arranging simple and straightforward content at the beginning and more difficult, complex, and integrated content later on aligns with these cognitive design principles. Such an approach is likely to minimize the cognitive load on learners that could result from the order of course material.
The cognitive teaching strategies and principles presented discussed herein have several implications for medical education. The first implication concerns the teaching method. By incorporating these findings into their teaching and curriculum development, medical school professors could potentially reduce the cognitive load on learners that may result from ineffective teaching methods or the curriculum itself. Supporting this notion, Lange et al. [36] discovered that students experienced a higher extrinsic cognitive load due to ineffective teaching methods and unclear instructional guidance. Further research has indicated that when instructional design is effectively implemented, it can minimize students' extrinsic cognitive load, allowing them to concentrate on learning activities that contribute to the construction of knowledge [37,38]. The second implication relates to the direction of education. Cognitivism aligns with the objectives of medical education by focusing on the development of thinking skills rather than the mere transmission of knowledge. Consequently, cognitive learning theory emerges as a significant educational theory that warrants ongoing research and application in medical schools. In a similar vein, Papa and Harasym [39] assessed the relevance of cognitive learning theory in medical education from the paradigm perspective. They anticipated that, in the future, a curriculum based on cognitive science could be developed to address deficiencies in the current curriculum. They envisaged a shift from the present knowledge-centered education to one that emphasizes the cultivation of higher-order thinking abilities, driven by advancements in cognitive science-based curriculum development.
A limitation of this study is that the cognitive teaching strategies presented are generalized to be applicable across various classes, irrespective of content. Consequently, the study does not offer specific cognitive teaching models tailored to particular content or objectives, such as models for meaningful conceptual learning or problem-based learning models for improving studentsŌĆÖ problem-solving abilities. This approach was chosen because I believe that outlining teaching strategies from a cognitive learning perspective is more straightforward and beneficial than detailing individual lesson models. Future research could provide great value by presenting content-specific lesson models for instructors interested in implementing targeted teaching methods like meaningful learning or problem-based learning within certain subjects. Additionally, this study could not showcase examples of all the cognitive strategies discussed due to the scarcity of reports on the practical application of these strategies in medical school settings. Future research should aim to supply exemplary cases of the seven teaching strategies outlined here, across various disciplines such as basic medicine, clinical medicine, humanities, social sciences, and skills training. This would offer valuable guidance for instructors seeking to integrate these cognitive strategies into their teaching. In summary, cognitive learning theory remains not a relic of the past but a highly relevant and practical instructional framework for medical education, both now.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



